

For most of the last forty years, a personal injury or mass tort firm trying to figure out what actually happened to a client medically had two options, both of them limited in fairly obvious ways. You could ask the client to remember, which is unreliable not because clients are dishonest but because nobody remembers their full medical history with the precision a case requires. And in personal injury especially, your client is often in the middle of an acute care crisis when you meet them. They are focused on getting better, on managing pain, on figuring out how to keep their life moving while they heal. Cataloguing every provider they have seen is not the work in front of them.
Or you could send authorization letters to every provider the client could name and wait thirty to sixty days for a chart to come back. Then, when those records arrived and surfaced providers the client had forgotten, you could send another round and wait another thirty to sixty days. And on the cases where the client could only describe the lab as “the one near the Starbucks,” you could open Google Street View, try to identify the building, and hope you were right.
That’s no longer the whole picture, and the shift is more significant than it sounds when you first hear it described.
A new layer of structured health data is now operationally accessible to plaintiff firms. It returns in minutes instead of months. It surfaces providers your client forgot to mention, diagnoses they didn’t know were billed in their name, prescriptions they don’t remember filling, and the prior injury they didn’t think was relevant to the case. It’s not a faster version of records retrieval, though it gets pitched that way often enough. It’s a different category of work entirely, and the firms that have figured that out are competing differently than the firms that haven’t.
It’s also worth saying upfront that this same data layer has been quietly accessible to defense counsel for years. The information asymmetry that’s shaped plaintiff PI litigation for a generation, where the carrier knows about your client’s prior treatment and prior claims before you do, is not structural to the litigation. It’s structural to which side has been working inside healthcare’s data infrastructure. That’s the part that’s changing in 2026.
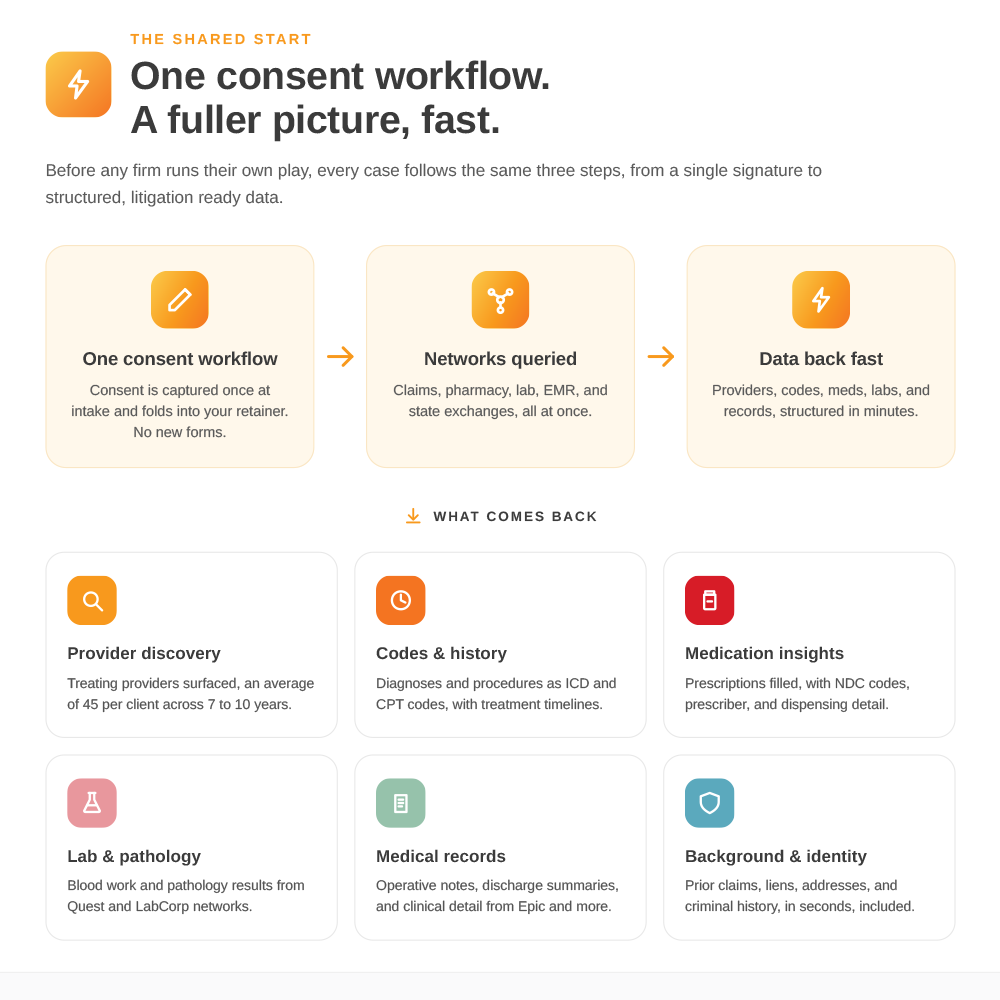
What follows is a working orientation to the layer: what it is, what it actually delivers in PI and mass tort cases, and how fast it returns.
What the new layer is
About eighty-five percent of U.S. health data is now digital, and it doesn’t live in any one provider’s filing cabinet. It lives in a network of operational systems that healthcare built for itself over the last two decades: claims clearinghouses that adjudicate insurance billing, pharmacy benefit management networks that authorize prescriptions, national lab networks that report results, state health information exchanges that move records between hospitals, and the major EHR systems that connect health systems across the country.
None of these systems were built for plaintiff firms. They were built for the operational needs of insurers, pharmacies, hospitals, and labs, which is part of why they work as well as they do. The data inside them is structured, queryable, and, with proper patient authorization, accessible to authorized parties.
A query against these networks doesn’t return a chart, and this is where the category distinction lives. A query returns a structured map of your client’s medical footprint: providers seen, diagnoses billed, prescriptions filled, labs drawn, with audit trails and timestamps. It tells you where your client has been. It does not, by itself, tell you what their treating physician wrote in the progress notes during their third post-op visit. The chart is still the chart, and retrieval still has its place, particularly for narrative content, certified copies for trial, and providers not yet in any digital network.
But the question retrieval was built to answer is “can you get me the chart for this provider,” and the question that comes first in a case is different. It’s “where has this client actually been, and what does the digital record say about it, before I’ve committed to a case theory.” That’s the question the new layer answers, and it’s a question retrieval was never designed for.
What it delivers in PI cases
For a personal injury firm, the operational gain shows up at three points in the case lifecycle, and it’s worth being concrete about each of them because the value reads differently depending on where you sit.
At intake, the new layer changes the economics of case selection. Full visibility into a prospective client’s medical footprint, returned within an afternoon, means you can see prior providers, diagnostic history, prescription patterns, address history, and background information before you commit any staff hours, vendor costs, or expert fees. The cases that should have been declined because of an undisclosed prior orthopedic injury, a previous PI claim, a prescription pattern inconsistent with the client’s account of their symptoms, become visible up front rather than three months in, when the work has already happened and the case has to be quietly walked back.
In pre-litigation, a complete medical picture lets you build demand calculations grounded in documented treatment history rather than estimated treatment history. A demand letter built on a complete record is harder to discount than one built on what the client could remember, and the case can settle earlier in the lifecycle if the carrier sees that the documentation is airtight from the start.
By the time you reach deposition, the same digital record defense counsel has had access to for years is available on your timeline, before opposing counsel sets the agenda. The deposition surprises that have shaped PI litigation for a generation, undisclosed prior treatment, prescription histories the client didn’t think to mention, providers the client genuinely forgot, are largely closable now. Not because clients are suddenly more reliable narrators of their own histories, but because you no longer have to rely on them being so.
What it delivers in mass tort cases
For mass tort firms, the use case sharpens further, because the layer is built for portfolio screening at volume in a way that retrieval simply cannot match.
You can configure tort-specific qualifying criteria, ICD codes for the qualifying injury, NDC codes for the implicated drug or product, exposure indicators relevant to the tort, and run an entire docket against the digital networks for proof of injury and proof of use. The output produces a qualifying list, a disqualifying list, and a flagged list of cases that need closer human review against criteria your firm sets.
For Roundup, that means oncology diagnoses and pathology codes. For PFAS, cancer diagnoses combined with elevated lab values and geographic residence history. For Depo-Provera, meningioma diagnoses and brain imaging records. For pharmaceutical torts more broadly, prescription history with NDC codes establishes both exposure and timeline, including the brand-versus-generic distinction that determines whether a case qualifies at all.
Mass tort firms running this workflow are reaching qualification decisions on thousands of cases at unit costs that weren’t possible three years ago, and reaching them before bellwether trial dates and filing deadlines force the question. The economics of mass tort intake have changed, and the firms that have rebuilt their qualification process around the new layer are running materially different docket math than the ones still relying on solicitation forms and self-reported intake.
How fast the layer actually returns
Speed is the easy thing to talk about, and probably the least interesting thing about what’s changed, but it’s also where the order of magnitude shift is most visible.
Claims and pharmacy data return in roughly five minutes per client. A nationwide background check returns in under thirty seconds. State health information exchanges return inside a couple of days. Major EHR system queries return in five minutes to five days, depending on the health system. A nationwide provider history returns inside twenty-four hours and typically surfaces forty to eighty providers per client, which is to say, considerably more than your client is going to remember at intake.
What used to take a records department thirty to sixty days per provider, multiplied across the providers a firm could identify, returns in an afternoon for the providers a firm didn’t know existed. That’s not retrieval running ten percent faster. It’s a different operational rhythm, and once a firm has been running on that rhythm for a few months, it’s hard to go back.
The leadership conversation
The new data layer changes intake. It changes pre-litigation. It changes deposition prep. It changes mass tort qualification. The firms that have built their processes around it are seeing fewer cases waste committed resources, more depositions go forward without surprise, and demand letters built on documented history rather than estimated history. None of that is hypothetical, and none of it requires abandoning a records team that’s already doing skilled, important work. The two layers are complementary, and a firm running both well treats them as one architecture.
The category distinction is the leadership-level call. Once a firm names the new layer for what it is, separate from retrieval, with its own place in the workflow, its own cost benchmark, and its own success metrics, the rest follows.
Talk to your team about how this changes intake. The firms that name the layer correctly are going to spend the next few years pulling away from the firms that don’t.
.svg)