
You’re forty minutes into a deposition. Your client is presenting with no pre-existing injuries or pain, and everything is attributable to the accident in question. Then defense counsel reaches into a folder and slides a printout across the table. Three prescriptions for a controlled-substance pain medication, written by a doctor your client never mentioned, filled three months before the accident at a pharmacy two zip codes from her house. Your client stares at it and says oh yeah that was for my bad back. You start recalculating in your head. Defense counsel gives the smallest possible nod. They’ve been waiting all morning to do exactly that.
Every trial attorney has a version of this story. The drug changes. The injury changes. The pattern does not. By the time that document hits the record, the defense has already built its strategy around it. You’re responding. They’re driving.
The asymmetry isn’t a function of cleverer defense work. It’s structural. For years, defense counsel has had operational access to a digital health dataset that plaintiff firms simply have not.
What’s in their binder
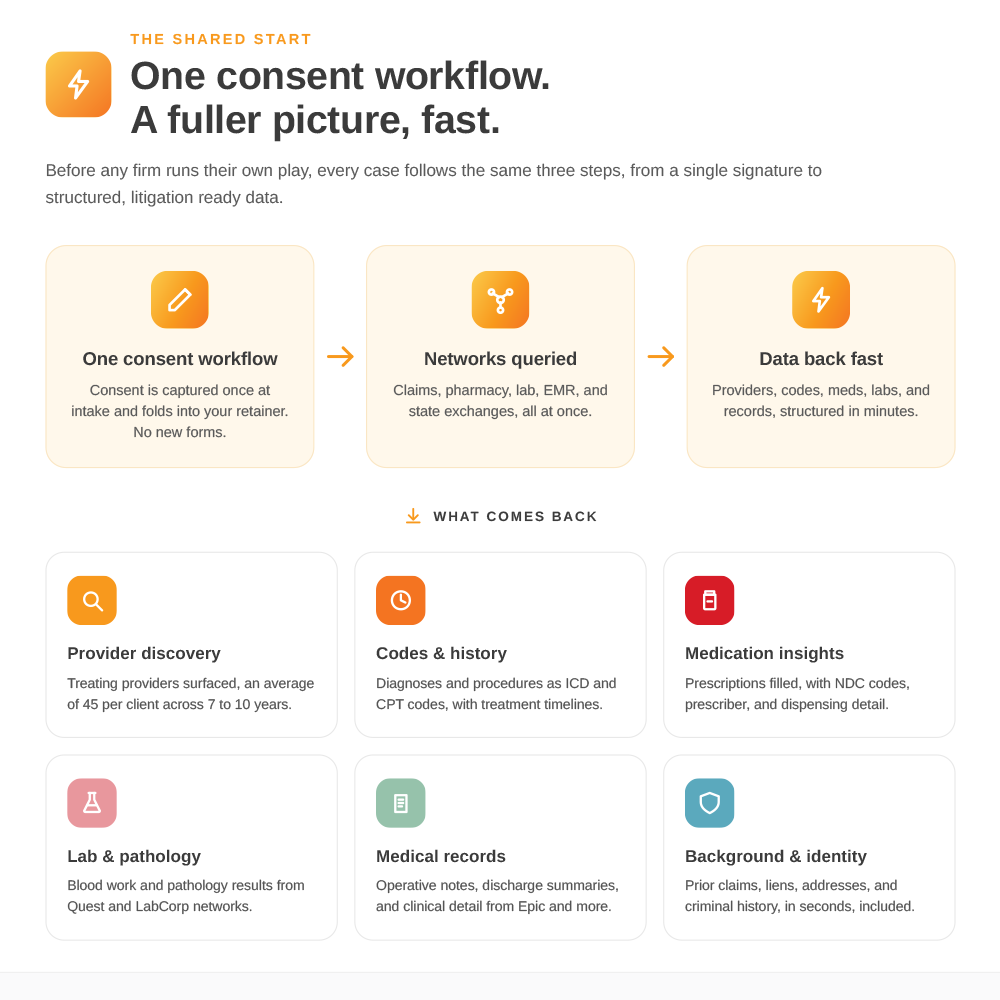
The U.S. health system has been digital for the better part of two decades. About eighty-five percent of health data now sits inside claims clearinghouses, pharmacy benefit management plans, lab networks, state health information exchanges, and EHR systems. Insurance carriers plug straight into the first three. Through those carrier relationships, defense counsel can ask a simple question before any deposition: does this plaintiff have an undisclosed provider, a prescription pattern that complicates damages, a treatment gap that breaks the timeline, or a pre-existing condition that reshapes causation?
The answer doesn’t come back as a stack of faxed paper from a single hospital. It comes back as structured data: ICD and CPT codes, NDC codes, lab values, provider lists. It returns in minutes, not weeks.
That’s what’s in the binder when defense counsel walks into your deposition. It isn’t magic. It’s access. And until recently, you didn’t have it.
What you’ve been missing
Traditional medical record retrieval works the way it has always worked. Name a provider, send a request, wait, get the file. It is essential. Certified court records, full clinical narrative notes, small private practices that don’t yet participate in digital networks. Those still come through the old channels, and nothing about digital data changes that.
But that workflow has one dependency it rarely admits: you have to already know who treated your client.
Your clients don’t always know. They forget the urgent care visit from three years ago. They forget the pain clinic they tried for a month and stopped going to. They forget the lab work ordered by a primary-care doctor they don’t see anymore. None of it is dishonesty. Memory just gets thin in exactly the places that matter most for damages: pre-existing conditions, treatment gaps, undisclosed providers, prescription history.
Digital health data fixes that gap by querying the same connected health network the defense is already using. Demographics in, structured medical history out. Claims data with hit rates of eighty-five to ninety percent on insured clients. Pharmacy networks returning near-complete prescription histories. Lab data covering roughly eighty percent of U.S. outpatient lab volume. State health exchanges that hand back every acute-care hospital record in a covered state for a single flat fee. The average client surfaces forty-five providers in the resulting picture. You see what the defense sees. The asymmetry collapses.
The surprises this kills
Pre-existing conditions sit in claims data months before the accident. Diagnostic codes, treating physicians, the specialty of the treatment. A back complaint from two years prior is no longer something the defense gets to introduce in your deposition. It’s something you’ve already addressed in pleadings, contextualized in the demand, and walked your client through under oath.
Pain-medication history sits in pharmacy data. Controlled-substance prescriptions, fill dates, prescribing doctors, dispensing pharmacies. Pharmacy benefit management plan data still returns Rite Aid dispensing records that are no longer obtainable through traditional channels since the bankruptcy. A pre-accident pain-management pattern is one of the most common deposition surprises in personal injury work, and one of the most preventable.
Treatment gaps live in the negative space of claims data. Defense counsel uses those gaps to argue the injury was less serious, or that some other event broke causation. Knowing the gap exists before you sit down lets you explain it on direct rather than absorb it on cross.
Undisclosed providers show up in the claims trail and in the provider list. Urgent care visits, specialist consultations, second opinions. None of those necessarily damage your case. All of them damage your case if the defense surfaces them first.
Lab and pathology results matter most where causation hinges on a specific finding: a cancer subtype, an exposure marker, a documented injury pattern. Defense counsel will already have those values. You walking into deposition with the same values are having a different conversation than you would be without them.
When to run it
The single most expensive mistake is running digital health data too late. By then you’ve committed to a case theory, and the value of earlier visibility is gone.
Pre-deposition is the right minimum threshold. Claims and pharmacy come back in about five minutes. Background data in less than one. State exchanges within a day. A query run two weeks before a deposition gives you a complete picture in time to fold it into your outline, your exhibits, and your client prep.
Pre-trial is also a defensible insertion point. A final query before you commit to the trial calendar catches anything new that surfaced since your last review, including providers seen after the demand and treatment that has continued during litigation.
The point
The deposition surprise is not a flash of defense brilliance. It is a function of structural access the plaintiff bar has not historically had. The access is now available. The firms that close the asymmetry stop walking into rooms where opposing counsel has read pages they have not.
Run a few cases through SettLiT before your next deposition. The version of yourself across the table will be glad you did.
.svg)