

You know the moment. You're in a deposition, the questioning is going your way, and then opposing counsel slides a document across the table. Records your client never mentioned. A prior injury to the same body part. A treatment gap that doesn't fit the timeline. A prescription history that cuts against your damages story. By the time you see it, the defense has already built their strategy around it.
That moment is almost always preventable. Not because you can predict every question, but because the information the defense is using was available to you too, before you ever walked into the room. The defense already has the printout. The only real question is whether you've read the same pages.
Here's the part that's easy to miss: most pre-deposition prep still runs on what the client remembers. And clients forget. They forget the urgent-care visit three years ago, the specialist their primary doctor sent them to, the medication they filled and stopped. They're not hiding anything. Nobody carries a complete medical history in their head. But the gaps in their memory quietly become the gaps in your prep, and the defense doesn't share those gaps, because they've been working from digital health data through claims relationships for years.
This checklist is meant to close that gap before you sit down. Think of it less as a sales pitch for any one tool and more as the set of questions worth answering about every client before a deposition.
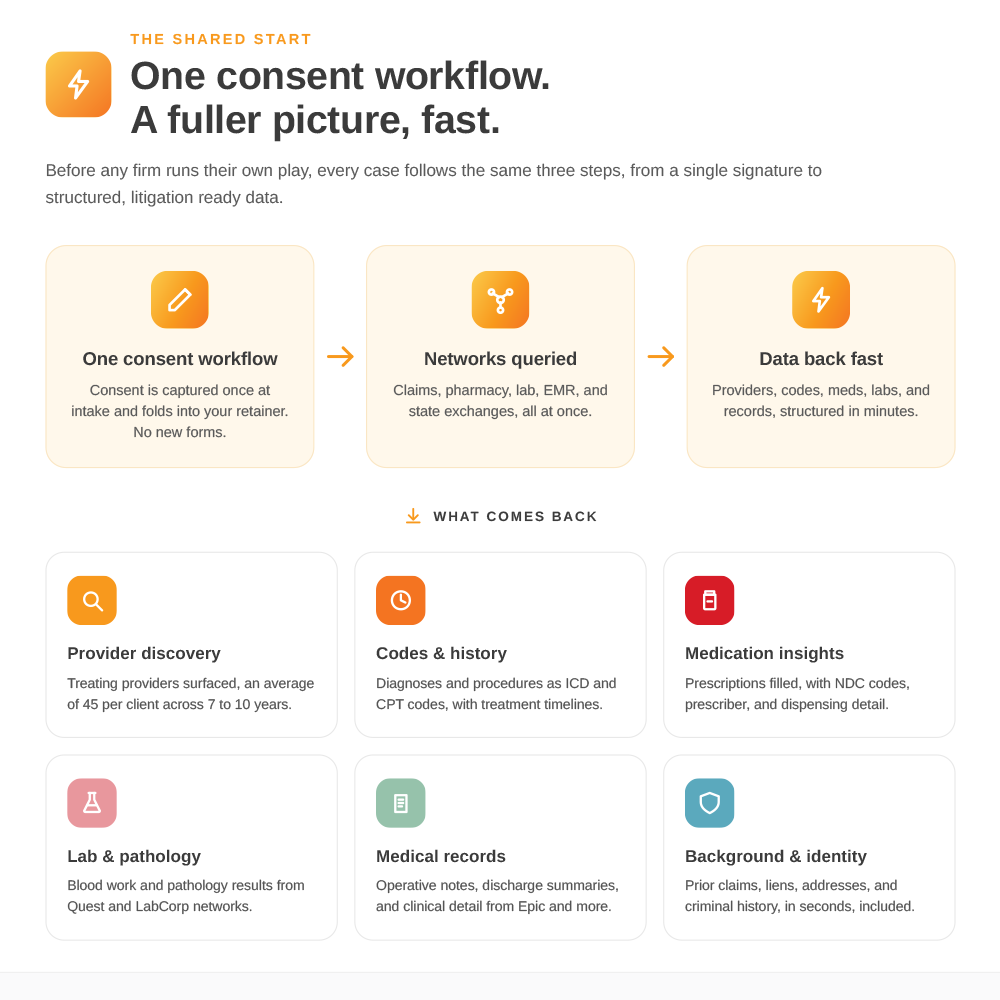
Before the deposition, confirm you can answer these
1. Do you have the full provider list, not just the ones your client named? A query across national digital networks typically surfaces around 45 providers, with specialties and dates of service. Some your client mentioned. Some they didn't. The ones they didn't are exactly where the defense goes looking, so that list is the foundation everything else builds on.
2. Do you know the pre-existing condition picture? Claims clearinghouse data comes back at an 85 to 90 percent hit rate, with diagnosis and procedure codes attached to dates. If there's a prior injury to the same region, a prior claim, or a chronic condition that predates the accident, it's far better to know now and prepare your causation answer than to hear it for the first time on the record.
3. Have you checked the medication history? Pharmacy network data returns at close to 100 percent for insured clients, including fill dates and prescribing physicians. Pre-accident pain management, controlled substances, anything the defense might frame as a competing explanation for the client's complaints: it's worth seeing before they raise it. (Keep any specific medication detail out of public-facing work product. Use it to prepare, not to publish.)
4. Are there treatment gaps you'll need to explain? A timeline with a six-week hole in it invites a hard question. If the data shows a gap, you can work through the explanation with your client in advance rather than watching them guess under oath.
5. Have you aimed your record requests at the right providers? This is where the digital picture earns its keep. Instead of sending 10 to 20 requests on guesswork and hoping the right charts arrive in time, you can use the provider list to send 2 or 3 targeted requests to the providers who actually matter. You walk in with the certified records that count, not a stack of irrelevant pages and three that never came.
6. Have you run the background check? Address history, prior claims, liens, criminal history. It comes back quickly, and it's the other place the defense looks for credibility problems. In one case, a firm found an undisclosed criminal history shortly before trial, reassessed, and resolved the case rather than walk into it blind.
Why timing is the whole point
None of this helps if it takes six weeks. Pre-deposition prep lives on a tight clock, and that's the trap traditional ordering sets: you request, you wait, and the records arrive after the deposition, or the morning of, with no time to absorb them. Most digital sources come back in about five minutes, with the full range running five minutes to five days depending on the source. That means the work fits the window you actually have, even when a deposition gets scheduled faster than you'd like.
It isn't magic. It's access: the same connected health network the defense already uses, available to you at the point where it can still change how you prepare.
What this doesn't replace
It's worth being clear-eyed about the limits, because overclaiming helps no one. This is digital-first, not digital-only. Coverage is real but not total. When you combine claims and pharmacy data, you'll see useful history for roughly 60 percent of clients, which means some providers, especially small private practices and anyone not yet connected to digital networks, won't surface. And the digital pull gives you structured data and clinical documents, not the certified narrative chart you'll ultimately enter into evidence. For that, you still order the record. The point isn't to retire your retrieval process. It's to aim it: the digital picture tells you where to look, and ordering delivers the authoritative document once you know.
The bottom line
The deposition surprise isn't bad luck. It's an information gap, and it runs in one direction, toward whichever side did the homework. Walk in having already seen the provider list, the pre-existing picture, the medication history, the gaps, and the background check, and there's very little left that can be slid across the table that you haven't already accounted for.
The records exist for both sides. Before your next deposition, it's worth the few minutes to read the same pages the defense already has.
.svg)