

Here is a scene every high-volume pre-litigation firm knows by heart. A client comes in with a soft-tissue injury from a rear-end collision. The story is clean, the presentation is credible, and your team signs the case the same week. Six weeks later the records start trickling back, and the picture changes: a prior back surgery nobody mentioned, two earlier claims for the same body part, a treatment gap that does not line up with the timeline you built the file around. By then you have already spent staff hours, vendor fees, and attorney attention on a case that looks nothing like the one you took.
The problem is not your intake team. The problem is that qualification has historically happened in the wrong order. For most personal injury firms, you commit first and learn later, because learning required the slow machinery of requesting records provider by provider. The client's own memory was the only data you had at the decision point, and a client's memory of their medical history is incomplete by nature. Nobody misremembers on purpose. They just do not carry an accurate ledger of every diagnosis, prescription, and provider they have seen over the past decade.
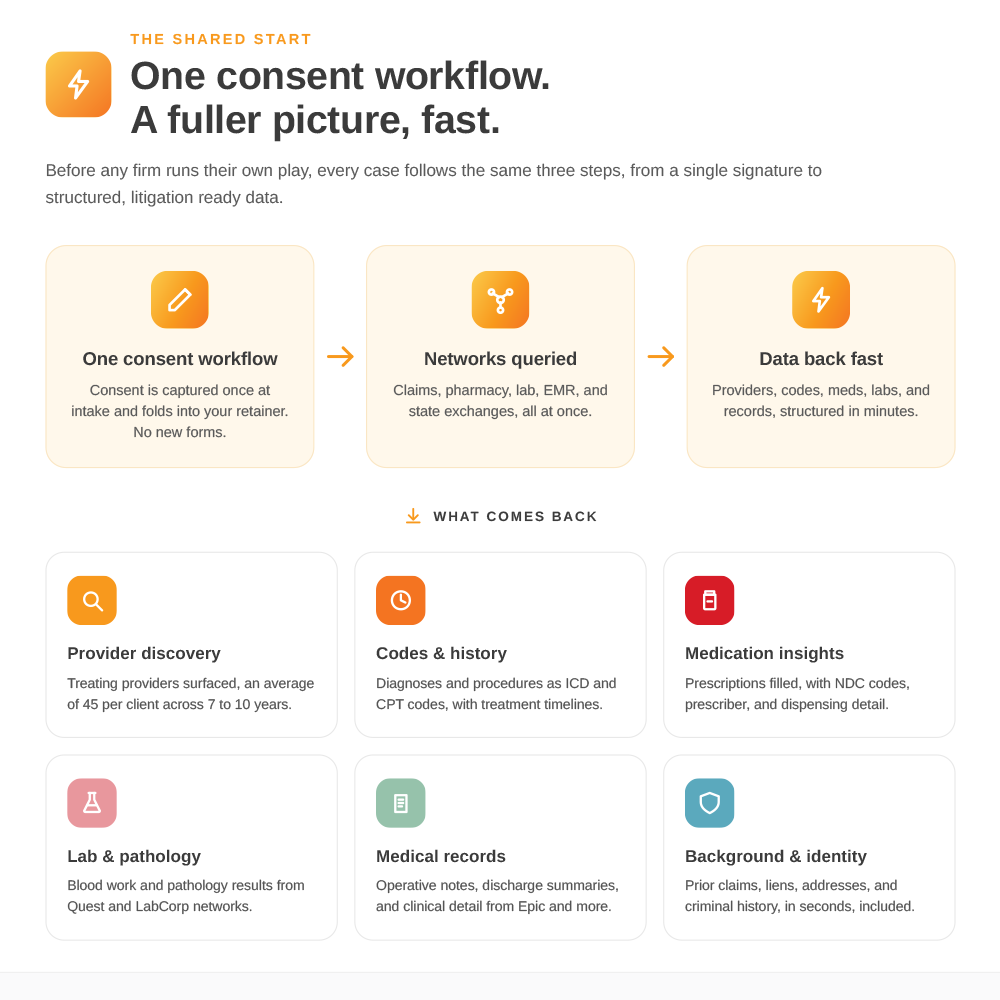
What has changed is that you no longer have to wait six weeks to find out who you actually signed. Roughly 85%of health data in the United States is digital and has been for over a decade, sitting in claims clearinghouses, pharmacy networks, lab systems, and state health information exchanges. With the client's authorization, those networks can be queried directly at intake. Claims data comes back in about five minutes with an 85 to 90percent national hit rate. Pharmacy history returns at a hit rate approaching100 percent for insured clients. A background check lands in under a minute.The full digital picture arrives before you have committed real resources, not after.
What “qualification” can actually mean now
Move the data upstream and the entire intake calculus changes. Instead of qualifying on a story, you qualify on a story plus a structured view of the client's real history. A single query surfaces, on average, 45 providers per client, including the ones the client forgot and the ones they would rather you did not find. You can see prior treatment for the same body part, a pattern of earlier claims, gaps that suggest the injury resolved before this incident, or pre-existing conditions that change how the case has to be built. None of this is a verdict on the client's honesty. It is simply the information you need to decide, with eyes open, whether and how to proceed.
The economics of this are straightforward, and they are what make it a pre-lit story rather than a trial story. Pre-lit firms run on volume and margin. The most expensive case you handle is the one you work for months before discovering it should have been declined or valued differently on day one. Decisions made without data are the most expensive decisions a firm makes, and at intake they are also the easiest to fix, because the cost of walking away is still close to zero. Spending a few dollars and five minutes to see the digital picture up front is cheap insurance against committing thousands downstream.
Qualification is not only about declining bad cases, either. It works the other direction. The same query that flags a problem case can confirm a strong one, surfacing treating providers you would not have known to chase and giving your team a head start on assembling the file the moment you decide to take it. You are not just filtering. You are starting the case faster, with a clearer map, for the cases you keep.
How it fits the intake workflow
The practical integration is less disruptive than firm operators tend to expect. The query needs a client signature on a patient data agreement plus basic demographics, name, date of birth, and ideally a prior address or two to sharpen the match. Most firms fold the authorization into their existing intake stack, so the client signs it at intake alongside everything else. No signature, no data, every time. There are several ways to place requests: a portal for manual entry and download, CSV upload for batches, and an API when you are ready to wire it into your case management system. Integrations with Filevine and Smart Advocate are available today, and a Litify integration is in development. You can start in the portal and graduate to automation later.
The sequencing that works best is a waterfall, and claims data goes first. Lead with claims at intake, then layer in the provider list and pharmacy data, all lower-cost, high-yield sources that map the territory in minutes. If the client lives in a state with a live health information exchange, that coverage is often the best value of all; in Nevada, for example, every acute-care hospital in the state is reachable for a flat $25 fee, frequently in about twenty minutes. Then, once you have decided to take the case, you point your traditional retrieval precisely at the two or three providers whose certified, complete charts you actually need, instead of firing fifteen requests into the dark. The digital layer makes the manual layer cheaper and sharper.
What it is, and what it is not
It is worth being precise, because overselling this to your partners helps no one. Digital health data is complementary to retrieval, not a substitute for it. You will still need traditional retrieval for certified court records, for full narrative notes in the clinician's words, and for providers that are not yet in digital networks.Coverage is real but not total: claims and pharmacy combined reach roughly 60%of clients, not all of them, and historical data generally goes back to the digitization era of the 2000s. The data returns billing and diagnostic codes rather than actual billed dollar amounts, which matters when you are building a demand around medical specials. The honest framing is digital-first, not digital-only. It gives you a strong head start at the decision point; it does not replace the file you build afterward.
There is also a trust dimension every firm should weigh, because the whole category lives or dies on it. This is compliance-first digital health data.Every query runs on patient authorization governed by HIPAA, with full audit trails, and is built to operate within the national health data infrastructure rather than around it. The platform's leadership co-chairs a Release of Information working group at DirectTrust and contributes to The Sequoia Project, and it was the first to gain legal access to the EpicChart Gateway. A SOC 2 Type II audit is expected to complete in May 2026.That governance is the reason the access is durable and the reason the audit trail behind your data holds up if it is ever questioned.
Rebuild the front door
For any firm, intake is the highest-leverage point in the entire case lifecycle, because it is where you commit resources you cannot fully recover. For years that decision had to be made on the thinnest information you would ever have about a client. That constraint is gone. The firms pulling ahead have rebuilt qualification around a simple principle: see the digital picture before you commit, not after. Five minutes at the front door changes which cases you take, how fast you start the ones you keep, and how much you waste on the ones you should have passed on.
Talk to your intake team about what it would take to put a query at the front of your qualification process, and run a handful of recent cases through it to see what you would have known on day one.
.svg)